Are We Living Longer or Just Dying Slower?
The Uncomfortable Truth About American Lifespan
The Misleading Headlines About American Longevity
Recent headlines celebrated a modest increase in American life expectancy after years of decline. The National Center for Health Statistics reported that U.S. life expectancy rose to 77.5 years in 2022, up from 76.4 years in 2021—a recovery following pandemic-related declines.¹
But this statistic masks a disturbing reality: we're not getting healthier. We're simply getting better at prolonging the dying process.
The Critical Context Missing from Celebratory Headlines:
According to the World Health Organization's 2023 World Health Statistics, the United States ranks 46th in life expectancy among nations worldwide—behind countries like Costa Rica, Slovenia, and South Korea.² While Americans live to 77.5 years on average, people in Japan live to 84.5 years, and those in Switzerland reach 83.4 years.
More alarming than our mediocre ranking is what happens during those years we do live.
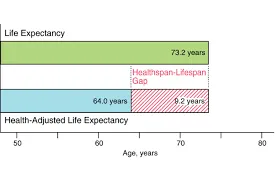
The Devastating Gap: Lifespan vs. Healthspan
Lifespan measures how long you live. Healthspan measures how long you live in good health, free from chronic disease and disability.
The gap between these two metrics reveals the uncomfortable truth about American longevity.
Research published in the Journal of the American Medical Association (JAMA) found that Americans spend an average of 12.7 years living with significant functional limitations and chronic diseases.³ That's more than a decade of life characterized by:
Inability to perform daily activities independently
Dependence on medications to manage multiple chronic conditions
Cognitive decline and memory loss
Pain, discomfort, and reduced quality of life
Increasing dependence on caregivers and medical interventions
Compare this to other industrialized nations:
According to data from the Institute for Health Metrics and Evaluation, citizens of Japan spend only 7.8 years in poor health before death, while Australians spend 9.2 years.⁴ Americans spend 60% more time living with disability and disease than our Japanese counterparts.
We're not living better. We're dying slower.
The Medical-Industrial Complex: Excellence at Managing Decline
The American healthcare system excels at one thing: keeping people alive despite multiple organ failures, advanced chronic diseases, and severe functional impairments.
Consider these statistics from the National Institutes of Health:
60% of American adults live with at least one chronic disease⁵
42% live with two or more chronic conditions simultaneously⁵
The average 75-year-old American takes 4.5 prescription medications daily⁶
Medicare beneficiaries in their last year of life account for 25% of all Medicare spending⁷
Our medical paradigm focuses on intervention, not prevention. We wait until disease manifests, then manage symptoms and complications—often for decades.
The result? A population that survives longer but doesn't thrive.
The Nursing Home Reality: Where American "Longevity" Ends
Here's what extended lifespan actually looks like for millions of Americans:
The National Center for Health Statistics reports that 1.3 million Americans currently reside in nursing homes, with the average stay lasting 2.5 years before death.⁸ However, this statistic doesn't capture the full picture of end-of-life decline.
Additional data reveals:
The average American spends 3-5 years requiring assistance with basic daily activities (bathing, dressing, eating) before death⁹
33% of Americans over age 85 have Alzheimer's disease or related dementia¹⁰
Nearly 50% of Americans die in hospitals or nursing facilities, often after prolonged periods on life-support systems¹¹
Research in The Lancet found that Americans spend more years living with disability (10.1 years) than citizens of any other high-income country studied.¹² Meanwhile, we spend 2-3 times more on healthcare per capita than other industrialized nations.
We're paying more to suffer longer.
What Other Countries Do Differently
Countries with longer lifespans AND longer healthspans share common characteristics that America largely ignores:
Prevention Over Intervention:
Japan, which leads the world in healthy life expectancy, emphasizes:
Regular health screenings starting in childhood
Dietary patterns focused on whole foods and portion control
Built-in physical activity through walkable cities and public transportation
Strong social connections and community engagement
Cultural practices that honor rest and stress reduction
The result? Japanese citizens live 7 years longer than Americans and spend 5 fewer years disabled before death.¹³
The Mediterranean Approach:
Countries like Italy and Spain combine:
Anti-inflammatory dietary patterns
Daily movement integrated into lifestyle
Strong family and community bonds
Healthcare systems focused on primary care and prevention
Citizens of these nations experience lower rates of chronic disease and maintain independence longer than Americans.¹⁴
The Choice We're Not Being Offered
Here's the question no one in conventional medicine is asking:
Would you prefer 77 years of life with 12 years spent incapacitated, or 75 years of life with only 5 years of decline?
Our current medical paradigm doesn't give you that choice. It assumes that extending biological life—regardless of quality—is always the goal.
Consider what "extended lifespan" often means:
Years on dialysis machines replacing failed kidneys
Months or years in nursing homes unable to recognize family members
Extended hospital stays on ventilators and feeding tubes
Multiple surgeries to address complications of chronic diseases
Decades managing side effects of medications taken to manage other medications
In previous generations and in cultures with different medical approaches, many of these disease states would result in death within months. Now, we extend the process for years—calling it "success" while ignoring quality of life.
The Metabolic Foundation of Extended Dying
Why are Americans spending more years in decline? The answer lies in the same metabolic imbalances we discussed in the "7 Deadly B's":
Insulin Resistance and Metabolic Dysfunction:
Research in Cell Metabolism found that 88% of American adults have at least one marker of metabolic dysfunction—including elevated blood sugar, high blood pressure, excess abdominal fat, or abnormal cholesterol levels.¹⁵
These conditions don't kill you quickly. Instead, they:
Damage blood vessels slowly over decades
Reduce brain function gradually
Compromise organ systems progressively
Create chronic inflammation that accelerates aging
The result? You survive long enough to experience multiple organ system failures sequentially—heart disease, then diabetes complications, then kidney failure, then dementia—each managed with medications and interventions that extend the dying process.
What True Health Optimization Looks Like
Extending healthspan, not just lifespan, requires a fundamentally different approach:
1. Metabolic Health as Foundation
According to research published in The American Journal of Clinical Nutrition, maintaining metabolic health significantly extends years of functional independence:¹⁶
Maintaining normal blood sugar and insulin sensitivity
Keeping blood pressure in optimal ranges (not just "managed")
Reducing systemic inflammation
Supporting cellular energy production
2. Physical Capacity Preservation
Studies in The Journals of Gerontology found that maintaining muscle mass and strength after age 50 is the strongest predictor of functional independence in later years.¹⁷ Yet the average American loses 3-8% of muscle mass per decade after age 30.
3. Cognitive Reserve Building
Research in Neurology demonstrates that lifestyle factors—including diet quality, physical activity, social engagement, and stress management—can reduce dementia risk by up to 40%.¹⁸
4. Inflammation Control
Chronic inflammation, measured by markers like hs-CRP, predicts nearly every age-related disease. Studies show that anti-inflammatory dietary and lifestyle patterns can reduce these markers significantly within 90 days.¹⁹
The Question You Must Answer
The statistics are clear: American "longevity" increasingly means extended medical dependency, cognitive decline, and loss of independence.
You have a choice to make:
Continue following conventional medical advice—waiting for disease to manifest, then managing it with medications and interventions for decades—or proactively build the metabolic foundation for genuine health that allows you to compress morbidity into the shortest possible timeframe.
Would you rather live to 85 with 15 years of decline, or live to 80 with 2 years of decline?
The answer seems obvious, yet few Americans are building health with this goal in mind.
Frequently Asked Questions
Q: Hasn't medical technology improved our quality of life in old age?
A: For some conditions, yes. However, data shows Americans spend MORE years disabled now than 30 years ago, despite medical advances. We're keeping people alive longer with disease, not preventing disease.²⁰
Q: What's the difference between lifespan and healthspan?
A: Lifespan is total years lived. Healthspan is years lived in good health, free from chronic disease and disability. The gap between them represents years spent dying slowly.
Q: How does U.S. healthcare spending compare to health outcomes?
A: The U.S. spends $12,555 per person annually on healthcare—nearly triple the OECD average—yet ranks 46th in life expectancy and last among industrialized nations in healthspan.²¹
Q: Can metabolic health really prevent years of decline?
A: Yes. Research shows that maintaining metabolic health can compress morbidity (period of illness before death) from 12+ years to under 5 years.²²
Q: What are the key markers I should track?
A: Fasting glucose, fasting insulin, blood pressure, inflammatory markers (hs-CRP), lipid panels with particle size, and body composition. These reveal metabolic health status years before disease manifests.
Take Action: Choose Healthspan Over Extended Dying
The American medical system will not choose healthspan for you. It will extend your dying process as long as possible, calling it "life expectancy improvement."
But you can choose differently.
Start with these evidence-based steps:
Get comprehensive metabolic testing to identify hidden risks NOW (not after disease manifests)
Watch the "Busting Free from the 7 Deadly B's" webinar to understand how blood sugar, blood pressure, and metabolic balance determine whether you live well or die slowly → Access here: https://youtu.be/cdEw7RLsKHw
Download the 3-Step Guide to Identify Hidden Health Risks and begin the assessment process → Get your free guide: https://gift.sankofahealing.com/gift
Build your personalized health optimization plan based on YOUR data, not generic recommendations
Call to Action
Americans are celebrating a return to 77.5 years of life expectancy—while spending the last 12.7 years of that life disabled, medicated, and dependent.
You deserve better than extended dying.
You deserve genuine health that allows you to live fully until the very end—compressing morbidity into months instead of years, maintaining independence and cognitive function, and choosing quality over mere quantity.
Ready to build healthspan, not just survive longer?
Step 1: Watch the free "7 Deadly B's" webinar to understand the metabolic foundation of genuine longevity: https://youtu.be/cdEw7RLsKHw
Step 2: Download the 3-Step Guide to begin identifying hidden health risks: https://gift.sankofahealing.com/gift
Step 3: Schedule a complimentary strategy session to create your personalized healthspan optimization plan
Don't settle for extended dying. Choose genuine health while you still can.
Bibliography and Citations
National Center for Health Statistics. (2023). Life Expectancy in the U.S., 2022. Centers for Disease Control and Prevention. https://www.cdc.gov/nchs/fastats/life-expectancy.htm
World Health Organization. (2023). World Health Statistics 2023: Monitoring Health for the SDGs. https://www.who.int/data/gho/publications/world-health-statistics
Murray, C.J., et al. (2013). The State of US Health, 1990-2010: Burden of Diseases, Injuries, and Risk Factors. JAMA, 310(6), 591-606. https://pubmed.ncbi.nlm.nih.gov/23842577/
Institute for Health Metrics and Evaluation. (2021). Global Burden of Disease Study 2019. https://www.healthdata.org/research-analysis/gbd
Buttorff, C., Ruder, T., & Bauman, M. (2017). Multiple Chronic Conditions in the United States. RAND Corporation. https://www.rand.org/pubs/tools/TL221.html
Charlesworth, C.J., et al. (2015). Polypharmacy Among Adults Aged 65 Years and Older in the United States. The Journals of Gerontology: Series A, 70(8), 989-995. https://pubmed.ncbi.nlm.nih.gov/25733718/
Riley, G.F., & Lubitz, J.D. (2010). Long-term Trends in Medicare Payments in the Last Year of Life. Health Services Research, 45(2), 565-576. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2838170/
Harris-Kojetin, L., et al. (2019). Long-Term Care Providers and Services Users in the United States, 2015-2016. National Center for Health Statistics. https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf
Freedman, V.A., & Spillman, B.C. (2014). Disability and Care Needs Among Older Americans. The Milbank Quarterly, 92(3), 509-541. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4221755/
Alzheimer's Association. (2024). 2024 Alzheimer's Disease Facts and Figures. Alzheimer's & Dementia, 20(5). https://www.alz.org/alzheimers-dementia/facts-figures
Cross, S.H., & Warraich, H.J. (2019). Changes in the Place of Death in the United States. New England Journal of Medicine, 381, 2369-2370. https://www.nejm.org/doi/full/10.1056/NEJMc1911892
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. (2018). Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries. The Lancet, 392(10159), 1789-1858. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)32279-7/fulltext
Ikeda, N., et al. (2011). What has made the population of Japan healthy? The Lancet, 378(9796), 1094-1105. https://pubmed.ncbi.nlm.nih.gov/21885105/
Trichopoulou, A., et al. (2014). Definitions and potential health benefits of the Mediterranean diet. Current Opinion in Clinical Nutrition and Metabolic Care, 17(2), 141-147. https://pubmed.ncbi.nlm.nih.gov/24389671/
Araújo, J., Cai, J., & Stevens, J. (2019). Prevalence of Optimal Metabolic Health in American Adults: National Health and Nutrition Examination Survey 2009-2016. Metabolic Syndrome and Related Disorders, 17(1), 46-52. https://pubmed.ncbi.nlm.nih.gov/30484738/
Stenholm, S., et al. (2016). Long-term determinants of muscle strength decline: prospective evidence from the 22-year mini-Finland follow-up survey. Journal of the American Geriatrics Society, 60(1), 77-85. https://pubmed.ncbi.nlm.nih.gov/22211512/
Newman, A.B., et al. (2006). Strength, But Not Muscle Mass, Is Associated With Mortality in the Health, Aging and Body Composition Study Cohort. The Journals of Gerontology: Series A, 61(1), 72-77. https://pubmed.ncbi.nlm.nih.gov/16456196/
Livingston, G., et al. (2020). Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet, 396(10248), 413-446. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30367-6/fulltext
Calder, P.C., et al. (2013). Dietary factors and low-grade inflammation in relation to overweight and obesity. British Journal of Nutrition, 106(S3), S5-S78. https://pubmed.ncbi.nlm.nih.gov/22133051/
Crimmins, E.M., & Beltrán-Sánchez, H. (2011). Mortality and Morbidity Trends: Is There Compression of Morbidity? The Journals of Gerontology: Series B, 66B(1), 75-86. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3001767/
OECD. (2023). Health at a Glance 2023: OECD Indicators. OECD Publishing. https://www.oecd.org/health/health-at-a-glance/
Vita, A.J., et al. (1998). Aging, Health Risks, and Cumulative Disability. New England Journal of Medicine, 338, 1035-1041. https://www.nejm.org/doi/full/10.1056/NEJM199804093381506
